From vaccine hesitancy to misunderstanding and misinformation, we look at why UK targets for public vaccination are being missed.
At the beginning of 2022, as the UK began to emerge blinking and unsteady from the lingering lockdown restrictions, the feeling was palpable that the launch and delivery of the various COVID-19 vaccines had been a potent demonstration of the positive power of public vaccination programmes and the science that underpins them. Developed, tested and approved in record time, more than 128 million doses of the Pfizer, Moderna and Oxford/AstraZeneca vaccines were administered in England alone between December 2020 and September 2022. Yes, some people had been hesitant about the receiving the jab – and others had been outright hostile – but for the vast majority the vaccines had, as promised, delivered the simple but strong relief of life getting back to normal.
However, far from this experience putting to rest any remaining doubts about the efficacy of vaccinations, the opposite appears to have happened. At the end of September 2023, the UK Health Security Agency and NHS Digital reported that the uptake rates for routine childhood vaccines in England were falling.
Wide of the mark
The headline was that vaccination coverage decreased in 2022–23: it fell for 12 of the 14 measures reported for the year, with decreases between 0.1 and 1.2 percentage points compared with the previous year. This meant that none of the vaccines met the 95% that the World Health Organization (WHO) targets. In fact, the last vaccination to achieve coverage above 95% was the 5-in-1 vaccine at age five, which hit 95.2% in 2020–21.
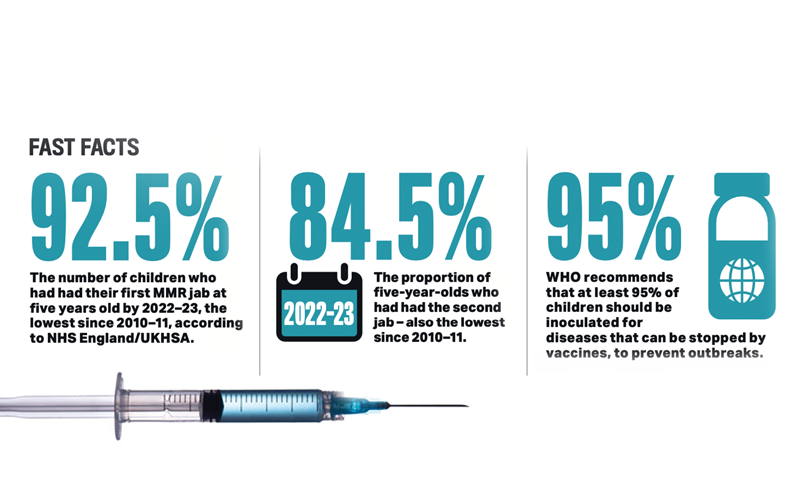
Among those vaccines failing to hit the 95% target was MMR1 (mumps, measles and rubella, first dose): its coverage at five years fell to 92.5%; MMR2 (second dose) coverage at five years fell to 84.5%; both were at the lowest level since 2010–11. MMR1 coverage at 24 months did actually go up marginally, from 89.2% in 2021–22 to 89.3%.
All coverage measures decreased at age five years: 5-in-1 coverage at five years had the largest year-on-year decrease in 2022–23, falling to 93.2%, the lowest level since 2008-09; Hib/MenC (Haemophilus influenzae type B and meningitis C) coverage also had its largest year-on-year decrease, falling to 90.4%, the lowest level since 2011–12.
A belt-and-braces approach

While these declines don’t appear substantial percentages, they make all the difference to the success of vaccines and the protection they can provide to the entire cohort. Dr Sarah Pitt, Principal Lecturer in the School of Applied Sciences at the University of Brighton, says it all comes back to the infamous R number, which was monitored so closely during the pandemic. “It’s a measure of the infectiousness of the organism. The R number for measles is between 12 and 18. It’s usually taken to be around 15, which means on average one child with measles could infect 15 other children. That’s super-infectious.”
This R number is vital for calculating the appropriate vaccination cover rate for all the individuals in the target population to ensure there’s enough protection to keep that R number below one. The calculation for measles comes out as 93%. In a belt-and-braces approach, a couple of percentage points are added to guarantee the coverage is more than good enough.
“It’s 95% for MMR simply because of the measles component,” says Pitt. “If it was just a vaccine for rubella on its own, we could probably get away with 75% or 80%.” In any combined vaccine, such as MMR, the threshold has to be high enough to provide protection against the most infectious organism.
If people haven’t seen what damage a disease can do, what reason do they have to fear it?
When that 95% threshold is met, the whole of that population is protected. Even though 5% have not been inoculated, their chances of being infected, for example, with mumps, measles or rubella are much smaller. But once that uptake figure drops below the threshold, the unvaccinated part of the population becomes vulnerable. But that unvaccinated population doesn’t necessarily consist only of those who have declined: there are also immunocompromised children who can’t have the vaccine and others who will simply get missed. No system is perfect.
“We’ve also seen that no vaccine is 100% effective in everybody,” says Pitt. “Part of that 5% is a proportion of people for whom the vaccine just doesn’t take, for whatever reason. It’s a known problem with hepatitis B and with rubella.”
Gaps beginning to show
Another potential reason for the declining uptake is that during the lockdown the routine vaccination programmes might have experienced some disruption and were perhaps overshadowed by the COVID effort. And with children not mixing at nurseries and schools, where, parents might wonder, was the urgency? A couple of years on, the gaps are beginning to show.
As these seemingly small dips in vaccine uptake can have big consequences for those who remain unvaccinated, and despite the historical success of vaccines in suppressing or even eliminating diseases, why are some people avoiding them?
“It’s partly the phenomenon of vaccine hesitancy, particularly in northern Europe, North America, Australia and New Zealand: what we’d call developed countries,” says Pitt.
Around the year 2000, the US was declared to be measles-free. It was a triumph for vaccination-based public health campaigns. But in 2015 an outbreak of the disease centred on the Disneyland theme park in California soon spread to several other states. The source was traced back to an unvaccinated 11-year-old. Subsequent studies suggested that up to half of the people exposed in that outbreak were unvaccinated, a consequence of widening vaccine hesitancy. Another outbreak in New York in 2018 affected the city’s Orthodox Jewish community, which had been susceptible to targeted misinformation – such tight-knit groups tend to be more likely to trust internal sources, even when inaccurate, than external authorities.
Both cases highlighted a growing problem, and when these small groups of people are added together, they become enough to drive vaccine uptake below the necessary thresholds. But what is at the heart of hesitancy?
“Perhaps one of the reasons is that people have become complacent,” says Pitt. “Look at diphtheria – who knows anyone who’s had diphtheria? Nobody, because we vaccinate children against it.” If people haven’t seen what damage a disease can do, what reason do they have to fear it? That’s especially true for measles. Though often talked about as a mild childhood disease, it can have severe consequences. “We have vaccinated children against measles for many years now, so few of them ever get the disease. Even doctors can’t diagnose it because they don’t see enough of it to tell the difference between that and any other sort of rash.”

Vaccine hesitancy
In 2019, WHO added vaccine hesitancy to its list of threats to global health (which also includes air pollution, climate change and antimicrobial resistance).
The key reasons it identified for hesitancy are complacency, inconvenience and lack of confidence.
An expert on the issue is Heidi Larson, Professor of Anthropology, Risk and Decision Science at the London School of Hygiene and Tropical Medicine, and founding director of the Vaccine Confidence Project (VCP).
Part of VCP’s work is to help individuals and communities make informed decisions about vaccines. It also collects the data for the EU’s State of Vaccine Confidence project. The 2022 report shows that overall confidence across the EU has dipped since 2020 and 2018. The headline statements and the percentage that agreed with them were as follows:
- Vaccines are important: 2018, 89.6%; 2020, 91.8%; 2022, 81.5%
- Vaccines are safe: 2018, 81.9%; 2020, 87%; 2022, 82.3%
- Vaccines are effective: 2018, 87.2%; 2020, 89.7%; 2022, 85.6%
In a 2021 interview, Larson outlined her insights into vaccine hesitancy: “It’s aligned with all kinds of ‘anti-control’ things … there’s an epidemic of distrust in the world, and governments haven’t done a lot to help us build trust. [People feel] left out of the decisions… some have told me they feel judged… just because they’re asking a question.
“We’ve also got to get rid of the language of ‘nutters’, ‘idiots’. The ones who are the most extreme are not stupid… then there [...] are genuinely concerned parents. We need to do a better job of listening.”
Misinformation can be stubborn
The MMR vaccination was also the subject of the Andrew Wakefield scandal in 1998. Despite the exposure of his fraud, which saw him struck off the medical register, misinformation can be stubborn, as Alastair Gammie, Global Director at Ortho Clinical Diagnostics, found. “I went for my flu vaccine the other day and the practice nurse told me that the parents of today’s young mothers are saying ‘Be careful about the MMR.’ A lot of these people didn’t do the vaccine when the rates were high enough, so they haven’t see any outbreaks or what measles can do, and they are advising their children not to give their own children the vaccine because of what Wakefield said about autism.”
Nor has the COVID experience cut through the more stubborn and mistrusting resistance that often characterises hesitancy. “I thought it would cure some of that,” says Sarah Pitt. “People would think, this is why we need vaccines, infectious diseases kill. Instead they got scared and confused by the mixed messaging from governments. Unfortunately, a few medical professionals added to the mix.”
COVID vaccines
Gammie feels there was almost a lack of honesty about the COVID vaccination and what it could, and could not, deliver. “People who were vaccinated still got infected and ended up thinking that this vaccination doesn’t work.” In boosting the immune system so people could better fight the infection on their own, it would have prevented countless hospitalisations, but how clear was that message?
Other voices claimed that the vaccines couldn’t possibly have been tested properly. “Just look at the amount of data produced during the first six months of the clinical trials,” says Pitt. “Then with everybody across the world being vaccinated, we got years’ worth of clinical data. We knew it was safe, we knew it was effective.” Did governments and scientific leaders communicate that clearly enough and in the right places to the right people?
This hints at the potential tactics for pushing back against misinformation and helping people to overcome their hesitancy. “Knowledge, information and publicity are key,” says Gammie.
Any pro-vaccine messages also need to be expressed via the most appropriate channels. “We have to drive these messages across social media, possibly by the so-called influencers, because people no longer seem to trust the medics.”
One of the most vital messages, says Pitt, is to remind people of why we need vaccines and what they have achieved. “What an amazing difference they’ve made to all our lives in the 20th century and beyond, and how important they are to protect us against infectious diseases. Without scaring people, we need to remind them what can happen if your child gets measles, and why we vaccinate against diphtheria and hepatitis and other diseases. And the reason we start early is to make sure that children get protection as soon as they need it, particularly pre-school.”
Explain and discuss
The consequences of falling vaccine rates and disease outbreaks need to be discussed more widely, says Gammie.
“We need to explain what a failed MMR or TB vaccine campaign would potentially result in, and help people understand that vaccinations have been well proven to be safe. The COVID vaccination was probably the largest trial ever run and while there were some side effects, considering the millions of people vaccinated they were negligible. This needs to be a message that gets through to young mothers.”
Just as important is how that message is communicated. Before the pandemic struck, Pitt was working with an immunologist colleague to explore via focus groups where the information mismatch is occurring – they are now looking to resurrect this work.
“We don’t know what’s going on in their heads. I do think some of it is that people are scared but we can’t just shout at them and say, ‘You are wrong – vaccines are great.’ That hasn’t worked. The real-life example of COVID hasn’t worked. It’s a question of trying to understand what they’re really worried about, then finding a way of reaching them and explaining the science and the benefits of the vaccine without putting them off.
“I don’t know how we reach them, but it’s important we do, for the sake of their own health and welfare and for the sake of others around them.”
Image credit | Richard-Gleed