Head of Pathology Services Consolidation at NHS Improvement, David Wells, sets out the progress made on the 29 networks and looks at the next steps and future plans.
As the NHS enters its 70th year, one constant has been the provision of universal healthcare, the other constant has been change. Change in approach, change in patients, change in technology, change in treatment and change in staff. Change for organisations as large and complex as the NHS is challenging. In pathology it has been long known that the current configuration of services is inefficient and demonstrates variation in terms of cost and quality. When compared to international services we do not operate at the size and scale of other services meaning that we require more people and more expensive equipment to provide our services. Innovation and adoption of new methods and techniques takes longer and is adopted inconsistently across the country. This is all at a time when we have a demonstrable workforce shortage, when funding for capital equipment is becoming harder to secure and when adoption of new techniques to support personalised medicine is becoming an imperative to diagnose disease earlier and improve our patient outcomes. This lack of size and scale also means we operate with several single points of failure that impacts upon hospital and community care. The most recent report authored by Lord Carter of Coles for the Department of Health, entitled Operational Productivity and Performance in English NHS Acute Hospitals: Unwarranted Variations, demonstrated that this is true across healthcare not just in pathology. One of the biggest obstacles in driving change has been a clear national plan and comparative data. NHS Improvement was given the task to change that.
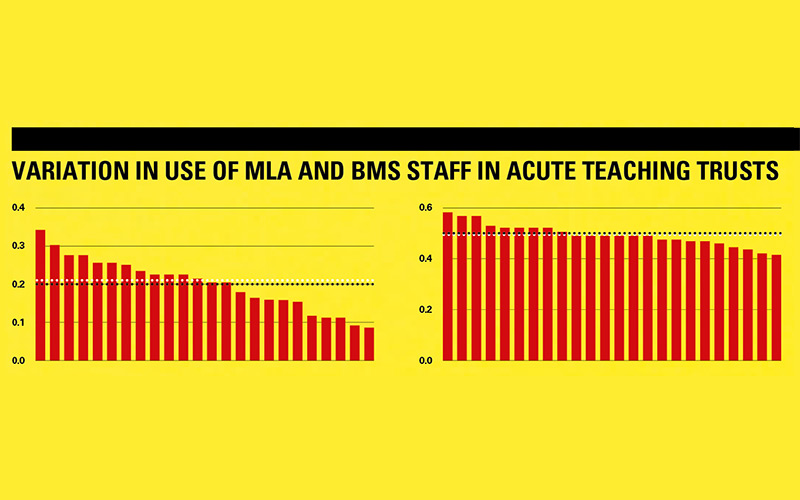
In September 2017, following the largest ever data collection undertaken in pathology services in England, NHS Improvement wrote to all acute hospital trusts, setting out a plan. The plan was to establish 29 pathology networks. These networks were modelled on the “Hub and Essential Services” laboratory approach. All hospital trusts, and later, all specialist hospital trusts were mapped into these networks and asked to form plans to deliver these changes. The data collected from providers (now available on Model Hospital, the online productivity and efficiency tool) show unwarranted variation in terms of pay and non-pay cost. This variation is not linked to size or type of hospital, however, can be linked to the service adopting best practice and innovative ways of working.
The benefits
One of the challenges to this change is for trusts to understand the clinical as well as economic benefit. We know that in some areas of diagnostics patients do not currently receive the turn-around time needed to adequately support their care. Networking can deliver these faster and more appropriate turn-around times.
Working in larger networks, patients – irrespective of where they live – should be able to access specialty expertise, which is not always available. Working at scale across networks can enable service resilience; consistent protocols, workforce, and equipment across multiple centres will ensure, in the event of a single laboratory being unavailable for whatever reason, there will be other laboratories capable of maintaining services. This scale can also ensure optimum equipment can be purchased, allowing laboratories to provide a wider repertoire of tests utilising the best methodologies. The latest sequencing technology or point-of-care testing (POCT) equipment purchased to serve a larger population is utilised more efficiently, meaning that business cases are more robust and more likely to be successful and, vitally, patients get access to the latest and best diagnostic tests and treatments. Interoperable IT systems with high levels of redundancy and immediate back-up and disaster recovery become affordable when serving multiple hospitals. We have seen a number of high-profile issues across the country, where IT systems have failed or back-up systems do not have the immediacy to provide seamless continuity, these failures have led to issues for service provision, and ultimately suboptimal patient care.
The greatest benefit is to the workforce. Training opportunities and advanced roles are more consistently available when services cover larger populations. The medical workforce in certain disciplines within pathology is in short supply and biomedical and clinical scientists are well placed to adopt new and innovative roles to not only enable networks to progress, but also to deliver a high-quality timely diagnostic service to patients. This is an opportunity to put into place the advanced roles envisioned by the modernisation of scientific careers programme and ensure all staff work to their top capability and competence.
Progress
Since the publication of NHS Improvement’s operational productivity report into the consolidation of 29 pathology networks, we have been progressing a number of workstreams to support providers in delivering the changes essential for sustainable, high-quality, clinically-focused pathology services in England. NHS Improvement has issued a number of toolkits to share learning, provide best practice advice and guidance. The Pathology team at NHS Improvement have been engaging with providers, arm’s length bodies, professional bodies and industry experts to ensure all parts of the system work together to support this change. This includes work that is on-going in genomics, antimicrobial resistance, screening, workforce, digital/AI innovations and other innovative disruptive technologies. This is to ensure the system makes one change to a truly interoperable system that will deliver on the national grand challenge to diagnose disease earlier and improve patient outcomes.
To date, over 80% of trusts are making progress towards networking their pathology services, others are going through the processes to enable them. To date, only two hospital trusts have found themselves unable to agree with the proposed model.
We continue to work with trusts, collecting and validating data, making some changes to the original networks or confirming the proposed configuration. We have completed our series of CEO workshops for most regions, these sessions have been very useful to all involved and have helped us move with pace in carrying out the work of modelling and forming networks.
During the year we also mapped specialist trusts into the 29 pathology networks with an ambition for them to work collegiately with other trusts locally, but also to work on a national level to ensure patients have access to expert clinical diagnostic services whilst supporting the sustainability of these services, recognising the challenges they face in training, recruitment, retention and adoption of new technologies.
The announcement in the spring by the Secretary of State for Health and Social Care awarding a total of £68m to organisations progressing projects networking their pathology service demonstrates the commitment to delivering this change to the sector. In addition to that, we have been working closely with the Office of Life Science to support the adoption, at pace, of the Life Science Industrial strategy for the benefit of our patients and the NHS.
Next steps
There is still much to do. Some networks move at pace, as named networks making ambitious plans for the future of pathology in their region, and existing networks embrace the “at scale” drive and have begun active discussions with other networks to see how they can deliver on a larger scale. Disappointingly, some networks are yet to get off the ground and some are not seeking to work at the required level of consolidation. These services are in the minority. The sector, both inside the NHS and industry, reports that, unlike previous pushes, the commitment to change is palpable. NHS Improvement will continue to support and monitor development of these networks, feeding into the Care Quality Commission’s Use of Resources inspections, where trusts are not making progress in removing unwarranted variation in cost and quality. We are also exploring working with commissioners who ultimately buy pathology services to identify best price and quality supporting those that do network.
Committing to quality
NHS Improvement is charged with rolling out the national Pathology Quality Assurance Dashboard (PQAD) proposed by the Barnes review in 2012. This dashboard, which will be issued in the summer, will hold trust boards to account for the pathology service they provide to their patients. Measuring not only clinically appropriate turn-around times but also: adoption of NICE guidelines; number of training posts in the service; number of tests provided under ISO 15189; and how many community point of care audits performed, amongst other metrics. We have worked closely with the professional bodies to ensure these metrics are appropriate and relevant. Historically, creation of networks has not led to a deterioration in quality, we expect networks once transition is complete to be ISO 15189 accredited for all tests that are provided. This may mean consolidation of certain tests into specialists testing centres with the relevant clinical and scientific expertise.
Pathology Optimisation Delivery Board
As well as working with the aspirant networks, NHS Improvement hosts the Pathology Optimisation Delivery Board, chaired by the National Clinical Advisor for Pathology, Professor Adrian Newland and vice-chaired by the President of the Royal College of Pathologists, Professor Jo Martin. The board is attended by a representative from the IBMS and representatives of the other professional organisations of the Pathology Alliance, NHS England, Health Education England, and senior leaders from existing networks. The Board’s role is to hold us to account and provide expert advice to ensure creation of clinically safe and sustainable pathology services for the future. It is important that we, as well as individual trusts, maintain a high level of transparency through staff and system engagement to ensure successful change. We also work closely with the national unions, industry and UKAS to ensure the whole sector is informed of the changes.
Leadership
We are under no illusion of the challenge that the creation of 29 networks brings to trusts and staff. The networks will need to cover the needs of several hospitals, providing the services essential for patient care, reaching out into the community providing direct access diagnostic testing as well as introduce new and innovative approaches to pathology, such as digital pathology and personalised medicine. It is vital that the profession gets behind the change, providing the expertise to the local networks, identifying the needs and opportunities to ensure a high-quality good value pathology service. This presents the profession with a unique opportunity to develop not only new advanced clinical roles, but also new senior operational leadership roles for those prepared to take on the challenge.
The principles
All networks were modelled on the following principles:
Patient referral routes, population size (1.5m minimum to 2.5m maximum), existing partnerships, such as STPs (Sustainability and Transformation Partnerships) or existing networks and geography was also considered for certain networks.
The way the networks would operate would be for the local network to decide. Networks currently operating in England are either an alliance of partners working together, a public joint venture where one trust takes on the running of services for the other hospitals, or a private joint venture where a new provider runs the services for the networked hospitals.
All activity that is not required to support direct acute patient care would be done in one place for the whole network (either as a single hub or a disturbed hub).
Essential service laboratories will be just that, only services that are essential to support the acute delivery of healthcare will be available.
Future
Pathology has a huge part to play in supporting the future of healthcare in England. Pathology cuts across the traditional boundaries of primary and secondary care, it has the data that can drive clinical pathways and testing strategies. We will need to challenge traditional delivery models, such as employing POCT to support not only a personalised approach to medicine but also a public health imperative. It is encouraging that other devolved nations are following the progress of the 29 pathology networks carefully and have commenced similar programmes.
Image Credit | Richard Gleed