Following technical advances over recent years, Professor of Diagnostic Haematology Barbara J Bain looks at investigating suspected acute leukaemia.
At a glance
- The patient is likely to present with symptoms of anaemia, bruising, bleeding and fever.
- Blood film examination may be the first modality to suggest possible acute leukaemia when this has not been considered by clinical staff.
- Morphology permits a speedy diagnosis – either provisional or definitive.
When I started training in haematology in 1971 suspected acute leukaemia was assessed by morphology of blood and bone marrow, by cytochemical stains (myeloperoxidase, Sudan Black B, non-specific esterase and chloroacetate esterase) and by cytogenetic analysis. That was quite a long time ago and things have moved on somewhat. The major advances that have been made since have been in immunophenotyping and molecular analysis. So how do we investigate nowadays and why does it matter?
Clinical assessment
We start with the clinician – perhaps the patient’s GP or an accident and emergency department. The patient is likely to present with symptoms of anaemia (breathlessness and fatigue), bruising and bleeding and fever resulting from infection. In the case of a child with acute lymphoblastic leukaemia (ALL) there may also be bone pain. Examining the patient may reveal pallor, bruises, petechiae, hepatomegaly, splenomegaly and, in the case of ALL, lymphadenopathy. Particularly if there is monocytic differentiation there may be infiltration of the skin or gums. Many of these features are likely to lead to a request for a blood count and film.
Leukaemia Diagnosis
The sixth edition of Leukaemia Diagnosis by Barbara J Bain and Mike Leach is out now, published by Wiley. It is a practical reference on the principles of leukaemia diagnosis and classification that illustrates and explains in a user-friendly way how different laboratory techniques are used to achieve an accurate interpretation. To aid in reader comprehension, over 300 high-quality, full-colour digital images of abnormal cells in leukaemia and lymphoma are included, supplemented by histological, cytogenetic and immunophenotyping images. IBMS members can get a 20% discount when buying the book by using the promo code MED20 at wiley.com (expires 1 August 2024).
The biomedical scientist
The biomedical scientist is confronted with a blood count and film with some brief clinical details. Alarm bells may ring – anaemia, neutropenia, thrombocytopenia, a blast flag. Blood film examination is urgent and may be enough to confirm the diagnosis. Apparent thrombocytopenia should be confirmed, excluding factitious thrombocytopenia due to platelet aggregation and false elevation of the platelet count by fragments of leukaemic cells or by schistocytes. At this stage it is important to look for indications that urgent intervention is needed, particularly when acute promyelocytic leukaemia is possible, and whether
the platelet count is dangerously low. A haematology trainee or consultant should be contacted speedily. Other tests needed at this stage include a coagulation screen, fibrinogen and D-dimer, blood group and antibody screen and tests of liver and renal function including uric acid. Cytochemistry is now rarely practised, except in resource-limited countries.
Sometimes clinical staff do not suspect acute leukaemia and the blood count may show only mild anaemia and thrombocytopenia. The biomedical scientist needs to search diligently for blast cells (and lymphoma cells) including along the edges of the film and in the tail, when a patient has unexplained cytopenia. Neutrophil dysplasia can also be a clue to an underlying acute myeloid leukaemia (AML).
The medical staff
The medical staff will assess the film/count and the patient. The patient is likely to be admitted immediately. A bone marrow aspirate is generally done, even if there is little doubt that the patient has acute leukaemia. This is to provide a baseline blast count and for cytogenetic analysis. Patients are often transferred between hospitals, so if this is likely to happen, make sure you have stained enough films that some will be left at the referring hospital. Make sure that an iron stain is done on the initial aspirate of every patient. A trephine biopsy is important if there is a poor aspirate and gently rolling the core biopsy along a glass slide will provide material that can be stained and examined some days in advance of histology results becoming available. Immunophenotyping is now routinely employed – flow cytometry, or immunohistochemistry, or both. If you need to send a specimen to another hospital for immunophenotyping, make sure you send a film as well, as immunophenotyping should not be interpreted in isolation.
Immunophenotyping
Immunophenotyping is important to distinguish AML from ALL and also to recognise mixed phenotype acute leukaemia (MPAL). The treatment of these three groups of conditions is quite different. It can also help to recognise acute promyelocytic leukaemia (APL). Typically these cases are CD34-negative and HLA-DR negative. It should be noted that this immunophenotype can also be seen in AML with NPM1 mutated.
Molecular analysis
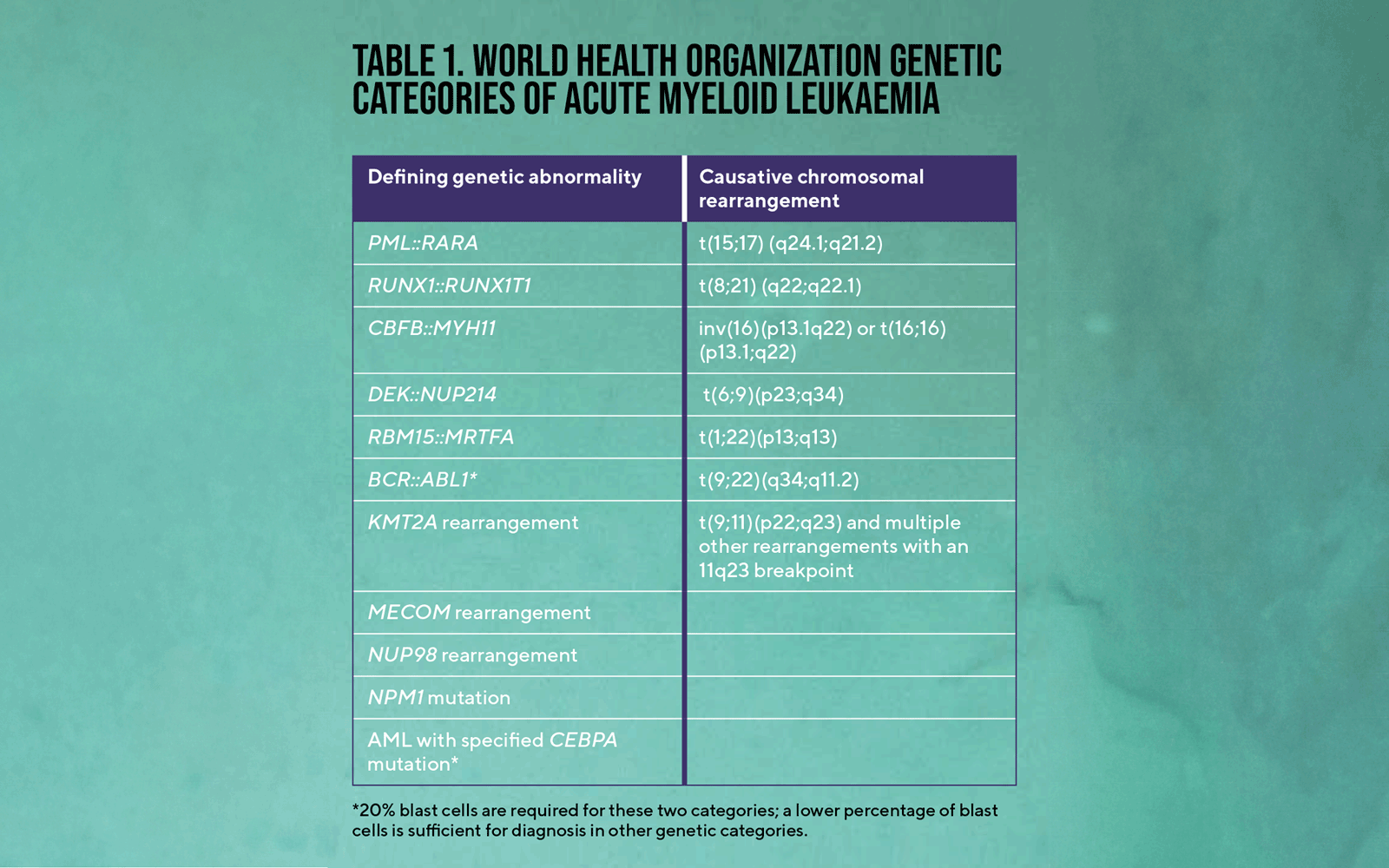
The 2020 WHO classification of acute leukaemias is firmly based on DNA analysis and specified genetic abnormalities take precedence over morphology. The molecular genetic lesion rather than a cytogenetic abnormality is used in the definition. Some genetic categories of AML are shown in Table 1. Only when cases have been assigned to these categories are residual cases classified on the basis of morphology and blast cell count. There is a sometimes conflicting 2022 International Consensus Classification that puts more emphasis on cytogenetic analysis. Acute lymphoblastic leukaemia is classified in a similar manner.
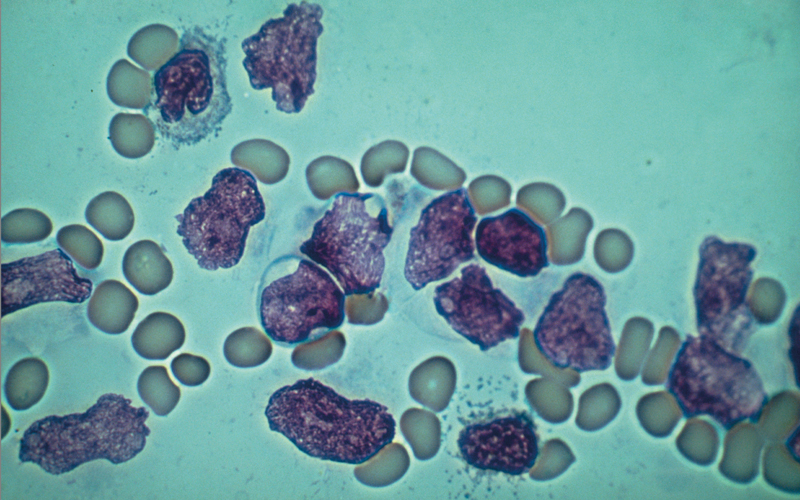
Top. Figure 1. Bone marrow film in classical hypergranular acute promyelocytic leukaemia showing hypergranular promyelocytes, one with a giant pseudo-Chédiak–Higashi granule. May–Grünwald–Giemsa (MGG) ×100 objective.
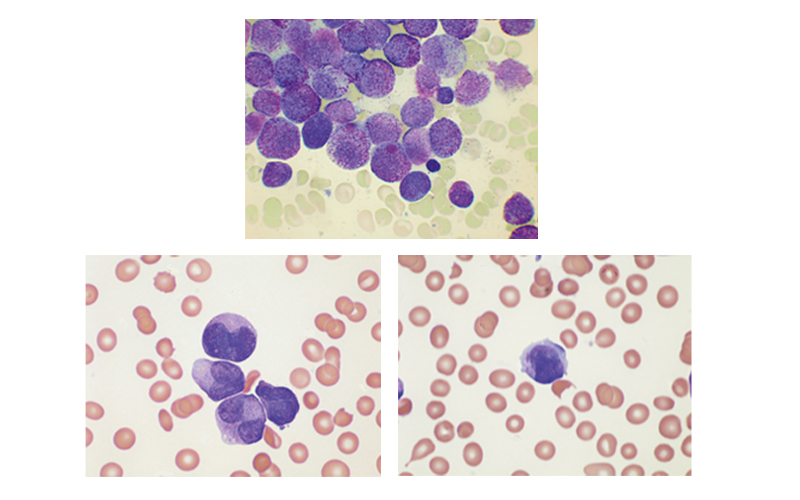
Below. Figure 2. Peripheral blood film in the variant form of acute promyelocytic leukaemia showing (a) the typical bilobed nucleus and (b) a leukaemic promyelocyte containing an Auer rod. MGG ×100 objective.
The purpose of classification
Immunophenotyping and genetic analysis of acute leukaemias are relevant for two reasons. Firstly, the information on lineage is relevant to choice of treatment. Secondly, it is relevant to prognosis and therefore to consequent decisions on the intensity and duration of treatment. Thirdly, certain genetic or immunophenotypic abnormalities may indicate the benefits of a specific targeted treatment. The optimal treatment for ALL, AML and MPAL differs, not only as to choice of drugs but also as to whether the possibility of central nervous system (CNS) or testicular disease needs to be considered. Imunophenotyping can reveal a specific target for treatment, as when expression of CD33 indicates the possible efficacy of gemtuzumab ozogamicin (Myelotarg) or expression of CD123 (seen in blastic plasmacytoid dendritic cell neoplasm) indicates the possible efficacy of tagraxofusp. Genetic information is relevant both to intensity of treatment and the likely efficacy of specific drugs. For example, ALL, AML and MPAL with BCR::ABL1 require tyrosine kinase inhibitors.
Mutations may be sought for classification and relevance to targeted treatment. For example, the availability of ivosidenib, an inhibitor of IDH1, and of enasidenib, an inhibitor of IDH2, makes detection of mutation or one or other of these genes potentially important for choice of therapy. There are also drugs available that target the prognostically adverse mutated FLT3 with an internal tandem duplication (FLT3-ITD).
Explore Further
Order the new edition of Leukaemia Diagnosis: bit.ly/43YLVbX
A podcast on morphology with Barbara J Bain: bit.ly/49lnvdA
Barbara J Bain’s page on ResearchGate: researchgate.net/profile/Barbara-Bain-2
The role of morphology
So is there a role for morphology given the wealth of immunophenotypic and genetic information now available? Blood film examination may be the first modality to suggest possible acute leukaemia. Morphology can often identify AML rather than ALL because of the presence of Auer rods or azurophilic granules although, in a minority of cases with very primitive cells, immunophenotyping is needed for lineage assignment. Morphology permits a very speedy diagnosis of APL. This is important because early death from haemorrhage can occur and urgent treatment with all-trans-retinoic acid and arsenic trioxide is indicated, without waiting for molecular confirmation. Recognition of the classical hypergranular form is relatively easy as long as there are leukaemic promyelocytes (Fig. 1) in the peripheral blood but recognition of the variant form requires awareness of the typical bilobed nucleus (Fig. 2).
Morphology sets one off along the right diagnostic pathway and permits a speedy diagnosis, either provisional or definitive.
Barbara J Bain is Professor of Diagnostic Haematology at the Centre for Haematology, Department of Immunology and Inflammation, Imperial College London.
Image credit | Science Photo Library