Louise Greenhalgh, a Specialist Biomedical Scientist in Cellular Pathology, presents a case study of a cancer with less than 50 examples reported in the literature.
The Higher Specialist Diploma (HSD) portfolio requires the completion of two case studies. These must follow the patient from presentation to treatment, through the pre-analytical, analytical and post-analytical phases. When completing a case study, it is important to take amultidisciplinary approach, documenting the considerations of both clinician and pathologist. Differential diagnoses must be discussed; patient history, alongside clinical and pathological findings, must be utilised to reach an accurate final diagnosis. The following case study was included in my HSD portfolio submission. I successfully gained my HSD in 2018.
Testicular tumours
A 65-year-old male presented with
a progressive, painless left testicular swelling. There was no history of trauma and no other genito-urinary symptoms. Upon hospital referral, the patient underwent physical examination, blood tests, ultrasound and computerised tomography (CT) scanning. Palpation revealed a hemi-scrotal swelling, consistent with a tense hydrocele. This is an abnormal collection of fluid between the two mesothelial layers of the tunica vaginalis and can arise from numerous events, including trauma, infection and testicular tumours. Since the patient had reported no trauma to the area and presented with no signs of infection, a testicular tumour was suspected as the most probable cause.
The most commonly encountered testicular tumours are germ cell tumours, which usually result in abnormal serum levels of alpha fetoprotein (AFP) or beta-human chorionic gonadotrophin (βhCG). However, germ cell specific markers for the patient were all within normal ranges. The patient did not fall into the usual age range for the more common germ cell tumours. Average ages for presentation of seminoma, yolk sac tumour, teratoma, embryonal carcinoma and choriocarcinoma are 30-40 years, 1-3 years, 10-30 years, 20-30 years and 10-30 years, respectively.
Ultrasound examination did not indicate a solid mass, as would be expected with most tumour types.
A cystic lesion with features suspicious of lymphoma was observed.
Primary malignant lymphoma of the testis usually occurs in patients over
60 years of age, fitting with the patient profile. Although the patient’s serum lactate dehydrogenase (LDH) level was within normal range, not all lymphomas present with elevated LDH levels.
CT scan of the chest, abdomen and pelvis was performed, with no significant intra-abdominal or mediastinal lymphadenopathy observed. No bony lesions were observed and organs, including liver, spleen, kidneys, pancreas and adrenal glands, were unremarkable. Left radical orchidectomy was performed under general anaesthetic and the specimen was sent to histopathology.
Examining the specimen
On gross examination, the specimen was described as an enlarged testis measuring 10x7x6 cm. The external surface and attached spermatic cord were unremarkable. Slicing at dissection revealed a thin walled, unilocular cyst, surrounded by a thin fibrous capsule and filled with thick chocolate coloured fluid. Multiple papillary excrescences were observed on the inner surface of the cyst.
At this stage, the pathologist commented that the macroscopic appearance of these papillary lesions resembled a mesothelioma, the most common malignant pretesticular tumour with an “epithelial” growth pattern, which usually occurs within the sixth or seventh decade. However, the papillary morphological features of the specimen unusually showed great similarity to those seen in borderline lesions of the ovary.
Microscopic examination confirmed the cystic nature of the lesion, with epithelium showing a serous lining, overlying ovarian type fibrous stroma. Multiple papillary tufts with branching architecture were observed. These tufts, lined by stratified columnar epithelium, had hyalinised fibrovascular cores. Mild nuclear atypia was noted, but mitosis and necrosis were absent. The epididymis was unremarkable, as was the spermatic cord. Stromal involvement and lymphovascular invasion were not observed.
The diagnosis
Differential diagnoses for testicular tumours with papillary pattern should include metastatic adenocarcinoma, primary adenocarcinoma of the epididymis or rete testis, Mϋllerian-type epithelial tumours and mesothelioma. As documented in previous publications, along with morphological appearance, the use of immunocytochemistry is essential for the differential diagnosis of testicular tumours.
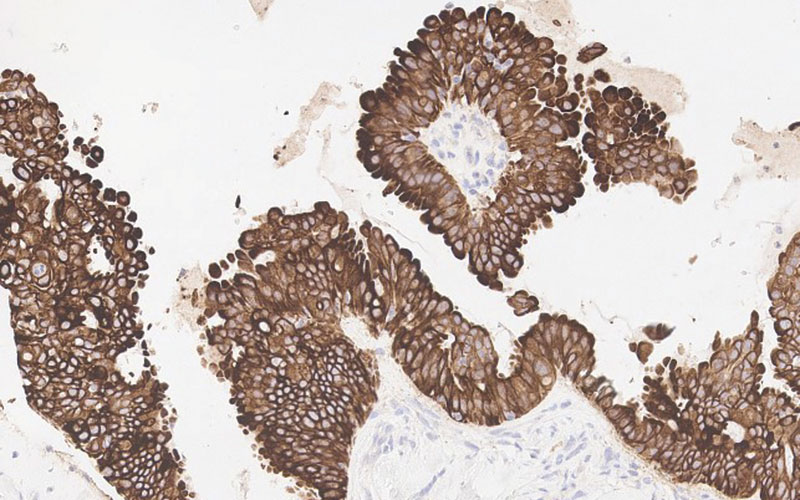
The epithelium of papillary tufts expressed cytokeratin AE1/AE3, CK7, CK5/6, WT1, CA125, PAX8, but not CK20, calretinin or carcinoembryonic antigen (CEA). The morphology and immunoprofile for this patient are in keeping with a diagnosis of ovarian type serous borderline tumour (SBT).
This diagnosis corresponds to similar reported case studies in the literature; all with patients presenting at similar age to this patient, with similar macroscopic and microscopic characteristics and identical immunocytochemical staining patterns. SBT of the testis is a rare tumour, with fewer than 50 cases reported in the literature.
Understanding
Prognosis and long-term implications for patients are not clear. Guidelines from The Royal College of Pathologists state: “Due to the rarity of testicular tumours, there are few randomised, large scale international studies of prognosis and outcome, especially in low-risk tumours.”
Continual surveillance is, therefore, required for this patient, who continues to have regular blood tests for CA125, βhCG and AFP, along with six-monthly monitoring CT scans. At the time of this case study, the patient remained an outpatient at the medical oncology unit.
The pathogenesis of SBT remains unclear. Several publications have suggested that the tumours develop from remnants of Mϋllerian ducts within the testis, while others support the theory of Mϋllerian metaplasia of the mesothelium of the tunica vaginalis testis. Several recent studies have demonstrated the presence of the BRAF V600E mutation in SBTs of the testis, that are also seen in similar tumours of the ovary, suggesting similar pathogenesis in both genders and strengthening the argument for Mϋllerian metaplasia theories. It is evident that further studies aimed at investigating the molecular pathogenesis and possible targeted treatment of these tumours, along with long-term patient follow-up is essential to increase our understanding of this rare tumour type.
Louise Greenhalgh is a Specialist Biomedical Scientist in Cellular Pathology, based at Lincoln County Hospital.