Associate Professor in Biomedical Sciences Paul Waller questions some of the assumptions made about point-of-care testing.

Point of care testing (POCT) is used in multiple settings (see Table 1), where it is presumed that rapid access to results will improve patient care; assumed benefits include reduced mortality/morbidity and length of stay, and improved patient convenience. It is this assumption that I wish to examine.
Estimates of expenditure on POCT are made using many different methods (Hortin, 2005; El-Osta et al., 2017) and so vary widely. Estimates range from 4% to 20% of the total pathology budget – about £200m to £1bn per year in the UK.
Despite this significant expenditure, evidence of the clinical effectiveness of POCT is scarce (Pecoraro, Germagnoli and Banfi, 2014; Verbakel et al, 2017). About 60,000 papers on POCT are published each year, of which only about 5% investigate clinical effectiveness (see Verbakel et al, 2017 for a comparison of clinical accuracy and clinical effectiveness).
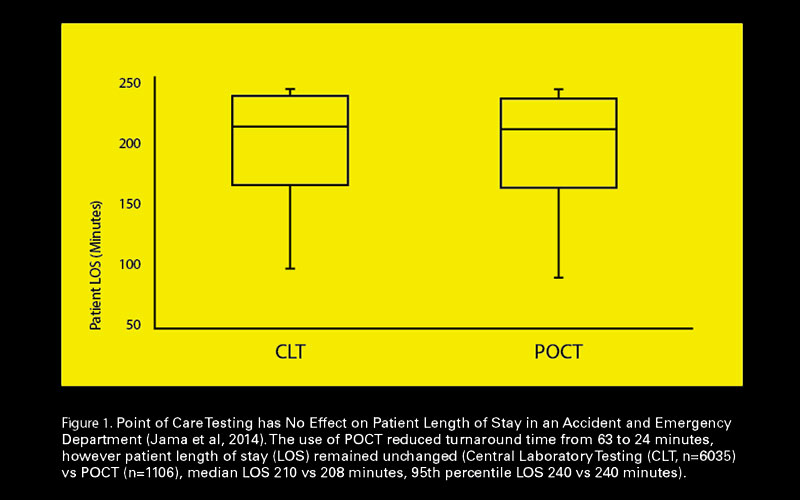
When clinical effectiveness is tested, POCT does not always produce the desired outcome. Three examples of this are illustrated in Figure 1 and Tables 2 & 3.
Why are we in this position?
There are two main reasons. Firstly, POCT is an “enabling technology” (Price and St John, 2012) and will not deliver innovation alone. Simple replacement of central laboratory testing with POCT will not necessarily change things. Secondly, although ISO15189 states that “management shall ensure that the laboratory participates in… activities that encompass… outcomes of patient care”, quality standards are more concerned with processes than outcomes (Barth, 2012).
The challenge
How should this situation be resolved? I suggest that two key principles should be applied. Proposals for the use of POCT should explicitly state what improvements are being sought (e.g. reduced length of stay, improved diabetic control, reduction in the number of outpatient visits), and demonstrate why POCT is necessary to enable these improvements. Pilot studies should fully test the use of POCT for its effectiveness before full implementation.
Healthcare scientists, diagnostics companies, clinicians, IT professionals and universities should collaborate to facilitate this testing, and results should be submitted for publication in peer-reviewed journals; adopting formal research practices provides excellent opportunities to study for research degrees, and research students can become a valuable manpower resource, helping overcome the workload issues that sometimes prevent this type of research being carried out.
Research will benefit all parties; diagnostics companies will be provided with evidence that their products are effective, hospital laboratories and clinical departments can be reassured that resources are being used safely and are improving patient outcomes, and universities will form valuable collaborative research relationships.
Paul Waller is Associate Professor in Biomedical Sciences at Kingston University. To see the references, view the article online at thebiomedicalscientist.net
Tables and figures
| Setting | Application | Assumed benefit |
| Home | Management of long term conditions e.g. diabetes, heart failure, anticoagulant monitoring | Better awareness of condition; motivation to manage condition; avoid need to attend hospital; avoid cost of transport; avoid time off work |
| High street pharmacy | Management of long term conditions; patient initiated testing e.g. flu test, strep A test, pregnancy test, cholesterol | Patient convenience; better access to relevant population; greater acceptance by patient; reduce need to visit GP; use when GP centre closed |
| GP surgery | Management of long term conditions; health checks | Improved long-term healthcare; reduced number of GP visits |
| Outpatients | “One-stop” clinics (e.g. diabetes, anticoagulant) | Patient convenience; reduced number of hospital visits |
| Ambulance | Pre-hospital testing e.g. cardiac markers, blood gases; Management of inter-hospital transport | Faster triage through A&E; earlier intervention; reduce risks of inter-hospital transport |
| Urgent care centres | Urgent care for non-life-threatening conditions; Rule-out testing | Avoid need to attend A&E; use when GP centre closed |
| A&E | Testing for rapid triage and treatment | Reduced length of stay in A&E |
| Theatre | Monitoring operative procedures | Reduce post-operative care requirement; convert to day care |
| ITU | Monitoring vital parameters | Improve mortality and morbidity; reduce length of stay |
| Monitoring (n=96) | Control (n=88) | ||
| HbA1c | 6.90% | 6.90% | No significant difference |
| BMI (% of baseline) | 97% | 99% | No significant difference |
| Proportion of patients taking hypoglycaemic drug | 64% | 59% | No significant difference |
| Event | Risk Ratio (self monitoring/testing vs standard monitoring (RR, 95%CI) |
|
Thromboembolitic events |
0.58 (0.45 – 0.75) |
| All cause mortality (self-management) | 0.55 (0.36 – 0.84) |
| All cause mortality (self-monitoring) | 0.94 (0.78 – 1.15) |
| Major haemorrhages | 0.95 (0.80 – 1.12) |
References
Barth, J. H. (2012) 'Clinical quality indicators in laboratory medicine', Ann Clin Biochem, 49 (1), pp. 9-16.
Bloomfield,H. et al. (2011) 'Meta-analysis: Effect of patient Self-testing and Self-Management of Long Term Anticoagulation on Major Clinical Outcomes.’ Annals of Internal Medicine 154 (7) pp. 472-482
El-Osta, A. et al. 'Does use of point-of-care testing improve cost-effectiveness of the NHS Health Check programme in the primary care setting? A cost-minimisation analysis', BMJ Open, 7 (8), e015494. doi:10.1136/bmjopen-2016-015494.
Heneghan, C. et al. (2016) ‘Self-monitoring and self-management of oral anticoagulation’ Cochrane Database of Systematic Reviews, 7 Article number .: CD003869
Hortin, G. (2005) ‘Does Point-Of-Care testing Save Money or Cost More?’ Laboratory Medicine 36 (8) pp. 465-467
Jama,L. et al. (2014) ‘Point of Care Testing Has No Effect on Patient Length of Stay in an Accident and Emergency Department’ Abstracts from the 3rd EFLM-UEMS Congress, Clinical Chemistry and Laboratory Medicine 52 (11)
Pecoraro, V., Germagnoli, L., Banfi G. (2014) ‘Point-of-care testing: where is the evidence? A systematic survey’ Clinical Chemistry and Laboratory Medicine 52 pp. 313–24.
Price, C., St John, A. (2012) ‘Point-of-Care Testing: Making Innovation Work for Patient Centered Care’ AACC (Washington, USA)
St John, A. (2010) 'The Evidence to Support Point-of-Care Testing', The Clinical Biochemist Reviews, 31 (3), pp. 111-119.
Verbakel, J. et al. (2017) 'Common evidence gaps in point-of-care diagnostic test evaluation: a review of horizon scan reports', BMJ Open, 7 (9), e015760. doi: 10.1136/bmjopen-2016-015760.



