Two years after the end of the most widespread Ebola epidemic in history and with a new outbreak in East Africa, what can we learn from those on the frontline?
In December 2013, an 18-month old boy called Emile Ouamouno died in the small village of Meliandou in Guinea, West Africa. He had been playing with the bats that lived in a tree stump a few metres from his home. Soon after his death, his sister and mother also died, and within four months the village had buried 14 of its residents.
Scientists have since reported that the bats were infected with Ebola.
But it was not until March 2014, when the virus spread to Liberia and then on to Sierra Leone, Nigeria, Mali and Senegal, that it started to garner global attention.
Fast-forward 21 months and the Ebola epidemic had officially claimed 11,315 lives, but with many deaths going unrecorded, some claimed the figure was up to three times higher.
As well as taking thousands of lives, the epidemic devastated already fragile healthcare systems and ravaged the economies of countries, some of which were still limping back towards recovery after a bloody civil war.
On 13 January 2016, the World Health Organization (WHO) declared the last of the countries affected, Liberia, to be Ebola-free. By this time the epidemic has killed five times more victims than all other know Ebola outbreaks in history combined.
The disease is now back. This time it has hit East Africa. From July to September this year, it claimed 85 lives in Congo and infected a further 39 people. Most of the victims were from villages and about 20 were from Beni, a city of several hundred thousand people with close links to Uganda. Then, on September 5, Peter Salama, the WHO’s Head of Emergency Operations tweeted: “Ebola case from Beni has died in Butembo, a city with close to 1 million people.”
As health officials struggle to control the virus’s spread through experimental vaccines and treatments, we hear the first-person accounts of two scientists who were on the frontline in 2014 and one who is involved in the current efforts to stop the East Africa outbreak escalating into another devastating epidemic.
Neil Bentley
Head of Technical Services for the National Infection Service, Public Health England
As part of the 473 volunteer scientists, I deployed to support the Ebola outbreak in West Africa within Sierra Leone between October 2014 and July 2016.
Our remit from the British government was to provide three laboratories with the capability to provide a molecular Ebola and RDT Malaria diagnostic service to support the outbreak. Latterly we also provided basic biochemistry and haematology diagnostics from each of the laboratories. Our laboratories at Kerry Town, Makeni and Port Loko were strategically placed within the Ebola Treatment Centres (ETCs) close to, but outside, large population areas.
My role was to help develop and lead the operational and technical laboratory service and organise a suitable in-country cold chain supply of reagents and consumables from the UK. Initially, this required us to work with the British military to help design and build the laboratories from scratch. This meant sourcing basic essentials, such as water and electricity, for the laboratories. There was significant pressure to open them as soon as possible and each initially opened while the ETCs were being built around us.
As the laboratories opened, it quickly became apparent that provision of diagnostic services was only a part of the public health requirements needed. There was also a requirement to train and develop local healthcare and support staff on how to effectively obtain patient samples and transport them to the laboratories as quickly as possible. We embarked on a series of community training and worked with the local transport teams to expedite sample delivery. These steps were particularly important, as any patient with a pyrexia (that can be caused for many reasons) was held within the Ebola holding centres, frequently for up to five days while waiting for laboratory results. Therefore, the probability of cross-infection while in these holding centres was significant. Our training and logistical support helped reduce the turnaround time from days to hours and hopefully significantly reduced disease transmission.
With laboratories, logistics and the public health running smoothly, we changed focus and worked with the Department of International Development, the Sierra Leone Ministry of Health and Sanitation (MOHS), NGOs and other international partners on measures required to control the outbreak. This involved helping with the coordination of laboratory and public activities at the national level, and included assessing viable technologies to help support diagnosis and public health.
My role within Sierra Leone continues, with assisting MOHS on the provision of a sustainable diagnostic laboratory service, and provision of effective public health and emergency response activities. This includes the building and refurbishment of three diagnostic laboratories at Makeni, Bo and in the capital city Freetown.
With personal hindsight, there are many things that we could have done differently. Namely reacting to this outbreak sooner, and by initially providing laboratory services out of tents while the ETC laboratories were being constructed. Locally we used traditional fluid balance and palliative medical techniques supported by state-of-the-art laboratory diagnostic services for the duration of the outbreak. Subsequent vaccine development, Ebola virus disease research and global changes in attitude will hopefully prevent outbreaks on this scale in the future.
Finally, Sierra Leone and its people will always have a special place in my heart, and, having been given an African name “Pa Bumba” (meaning rich old man), I will keep returning to try to make a difference.
Victoria Atherton
Senior Biomedical Scientist (Microbiology), General Hospital, Jersey.
Due to my day job, I had been following the West Africa Ebola outbreak in 2014 with interest. As a member of the Army Reserve, I was asked to attend a pre-deployment Ebola-specific training course. This was the first indication that I might be mobilised for Operation GRITROCK, I was excited at the possibility and also nervous of the challenges I may face.
In December 2014, I received my mobilisation papers. In January 2015, I left Jersey with a rucksack, kit bag and day sack, containing everything that I might need.
All the deploying Defence Medical Services personnel spent two weeks in York carrying out Ebola-specific training and getting familiar with the protective equipment. The training allowed everyone to get used to working together as a team. We then flew to Sierra Leone. I think we were all apprehensive, but at this stage probably more about our accommodation and the country itself, rather than the job. It was hot and I spent the next two and half months looking slightly pink and very shiny.
The laboratory in Kerry Town was split in two, with our colleagues from Public Health England performing the Ebola testing. The MOD staff performed full blood counts, biochemical profiles and other tests on Ebola-positive samples.
The laboratory was near a patient rest area and it was amazing to see those that survived get stronger before being discharged. Survivor ceremonies were performed, which involved a lot of dancing and singing. The defence medical personnel were accommodated at an old army camp, where the food was brilliant and we travelled to work each day in an old school bus. A lot of our free time was spent running and we also had film nights and quizzes.
Being in Sierra Leone at such a time was an amazing experience, I think we all hoped we had helped to combat a dreadful disease. We made some friends, had some laughs, worked hard and had a small insight into an interesting country with fascinating cultural links to the UK.
Claude Bandelier
Laboratory Manager, Médecins Sans Frontières
When Médecins Sans Frontières arrived in Mangina, the epicentre of the current Ebola epidemic in North Kivu, Democratic Republic of Congo, the local health centre was already full of confirmed and suspect patients, including many medical personnel who had been infected at work. We had to work quickly to improve the biosecurity of the isolation ward and simultaneously construct an ETC where the patients could be transferred and treated safely. With an initial capacity of 68 beds, the ETC received 37 patients the day it opened.
As a biologist, my role was to construct a secure laboratory inside the ETC in order to carry out biomedical analysis in collaboration with the Congolese Ministry of Health and the National Institute of Biomedical Research. The laboratory, set up under a tent, is equipped with a portable glovebox and is situated on the edge of the high-risk and low-risk zones.
The role of this laboratory is to quickly diagnose on site all suspected Ebola patients on admission to the centre, to be able to isolate the “positive” patients and refer the “negative” patients to a suitable health structure for further care. It also gives us the means to regularly monitor patients’ biological parameters in order to help assess their condition and adapt their care accordingly. The laboratory also provides diagnostic support to community health teams who swab the bodies of those suspected of dying of Ebola in the community in order to identify new hot spots of the outbreak.
I have worked with MSF on a previous Ebola outbreak and came to North Kivu to contribute my experience and learn more about Ebola. A difficulty in this epidemic is the geographic location. This time, Ebola has erupted in an area of active conflict between armed groups. Movement between villages and access to certain areas is restricted and difficult. Ebola is very difficult to predict. Constant care and attention is required, and it is difficult to know how the epidemic will evolve. It is very important to work closely and transparently with local people and to earn their trust. They must be informed about the virus and the response in order to accept the presence of international organisations. It is also important that equipment is developed to be more mobile and compatible with the constraints of the field.
With the difficult working conditions that come with an Ebola emergency, in terms of long hours, stress, constraints and emotions, we have also shared good times with the staff and community. Discharging cured patients is always very moving and rewards us for our work.
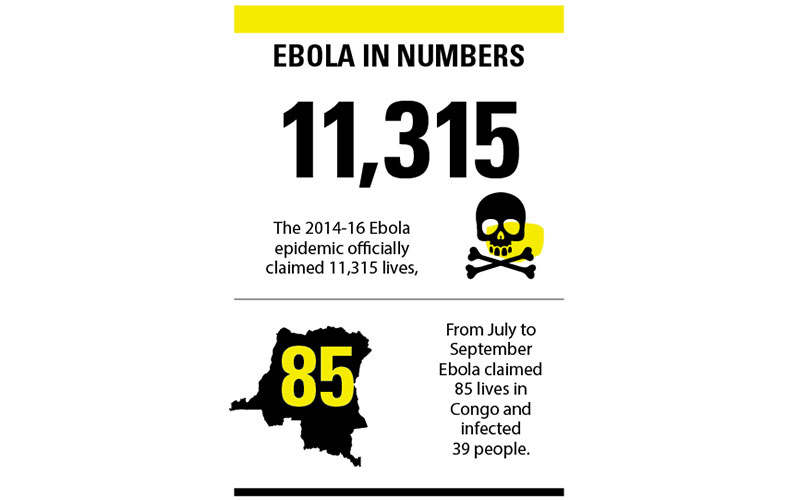
Image Credit | Getty/ iStock