Anaemia is identified by the World Health Organisation (WHO) as a widespread public health problem with major consequences for human health and social and economic development.

Affecting approximately two billion individuals, WHO estimates that almost 25% of the global population is affected by anaemia1.
Anaemia is one of the most common disorders of the blood, where the number of red blood cells and/or their oxygen carrying capacity is insufficient. This can impair quality of life and potentially lead to additional health complications or life-threatening conditions. There are multiple types of anaemia and a wide variety of causes. Diagnosing this complex disease therefore presents a challenge for clinicians to ensure the correct type and cause can be identified to direct the best treatment path.
The prevalence of anaemia
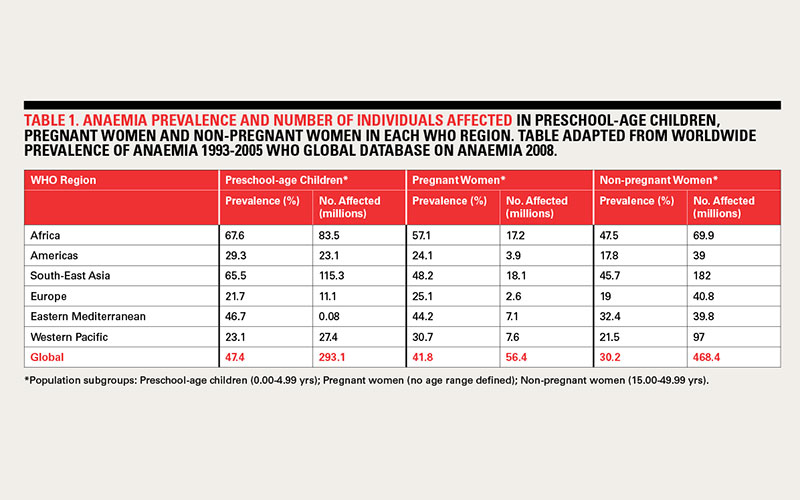
Global statistics on the prevalence of anaemia are difficult to obtain, however, the most recent report from WHO provides some figures that highlight the number of individuals affected across different regions (Table 1, below). In general, anaemia tends to affect vulnerable people, namely young children, pregnant women, the elderly, and people with serious and chronic diseases. The highest prevalence is in preschool-age children, while the lowest prevalence is in men2.
In developing countries, anaemia affects over half of preschool-age children and pregnant women, and is one of the most common, preventable causes of death within these groups3. However, anaemia is a worldwide issue, with figures for industrialised countries reaching 30-40%3 for these demographics as well.
In developed countries there is a high prevalence of anaemia among the elderly. For individuals aged over 50, a US study showed that anaemia prevalence rates rose rapidly to greater than 20% for those aged 85 and over4. As life expectancy continues to increase and the ageing population grows this creates an important health issue. When anaemia reaches a severe level, it is associated with fatigue, weakness, dizziness and drowsiness, and in extreme cases, death. Notably, surgical patients affected by anaemia can experience increased risk of postoperative morbidity and mortality5,6.
Challenges and complexity of anaemia
Despite the global prevalence and seriousness of anaemia7, it often remains under recognised and goes undertreated due to its complex nature and the fact that there are multiple specific types, all with different causes, implications and treatment options. Adding to the complexity, many of these different types can often coexist.
There are five main types of anaemia:
- Iron deficiency anaemia (IDA) – the most common globally
- Vitamin deficiency anaemia – e.g. Vitamin B12, folate & Vitamin A
- Anaemia of chronic disease (ACD)
- Anaemia of cancer
- Anaemia of renal failure
As each of these different types of anaemia has a different cause, it is important that clinicians are able to distinguish between them and correctly diagnose the accurate basis of a patient’s anaemia for treatment. Patients suffering with anaemia will often present with general and varied symptoms, which a clinician needs to interpret. To combat the complexity of anaemia and the challenges clinicians face reaching a diagnosis, a wealth of information is needed, compiled from a variety of laboratory tests.
Diagnosing anaemia – a comprehensive menu of testing options
Laboratory testing aids clinicians in diagnosing and pinpointing which type of anaemia a patient is affected by in order to direct the correct treatment.
In general, a clinician will first run haematology testing including a complete blood count and haemoglobin levels. These initial results help determine whether or not a patient has anaemia. Following this, additional testing is available to confirm the cause of anaemia depending on a patient’s history, clinical symptoms and results from previous tests.
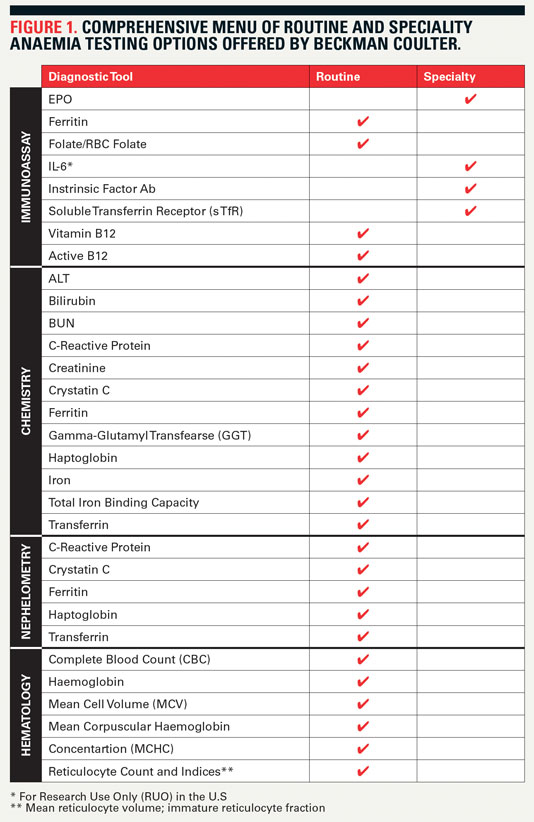
Valuable anaemia-related diagnostic information can be obtained from a wide variety of laboratory tests. Providing the most comprehensive offering of anaemia tests available, Beckman Coulter supports clinicians with greater insight into their patients’ conditions and offers more pathways to improving patient care. This range includes 28 different tools (Figure 1, below) that cover a variety of laboratory disciplines – haematology, nephelometry, chemistry, and immunoassay. Results from these tests deliver comprehensive, accurate information for effective diagnosis, treatment and monitoring for adjustment of anaemia therapy.
Focus on Active-B12 aka HoloTC
Supporting the diagnosis and monitoring of vitamin deficiency anaemia, the latest addition to Beckman Coulter’s range of anaemia testing options is the Access Active B12 assay. Vitamin B12 deficiency is widespread and can heavily influence patient health; it is directly linked with the megaloblastic anaemia known as pernicious anaemia8.
Vitamin B12 itself – also known as cobalamin – is an essential nutrient found in people’s diets in meat, fish, and dairy. Deficiency in vitamin B12 is therefore often seen in individuals who consume little or no animal products. It is also prevalent in the elderly9, pregnant women and patients with renal or intestinal conditions. As the neurological symptoms of vitamin B12 deficiency can be unspecific and irreversible, it is crucial to detect it early8.
The transportation of vitamin B12 around the body involves three binding proteins – Intrinsic Factor (IF), transcobalamin (TC) and haptocorrin (HC) – which enable the efficient uptake of the small amounts of vitamin B12 available from an individual’s diet. When TC and HC bind with vitamin B12, the resulting complexes are known as holotranscobalamin (HoloTC) and holohaptocorrin (HoloHC). HoloHC accounts for the major fraction of vitamin B12 in the circulation, representing 70-90% of vitamin B12 in the blood. However, it is biologically inert. HoloTC is the only active form of vitamin B12 that can be taken up by cells, but only accounts for 10-30% of vitamin B12 in the blood. It is therefore often termed Active-B12.
Traditionally, serum B12 testing measures total circulating B12 (HoloTC plus HoloHC). It therefore doesn’t provide a totally accurate representation of the vitamin B12 available to the cells in the body. The Active-B12 assay measures the critical form (HoloTC), and can be used either as a first line test for screening patients and determining their vitamin B12 status, or as a resolving test. In this case, clinicians may choose to continue using total B12 testing initially and then follow this up with Active-B12 testing should the results be indeterminate – a common occurrence with total B12 testing. In both situations, studies have shown that using the Active-B12 test provides a more reliable and earlier indicator of B12 deficiency. The test runs on a routine analyser and so it is easy to implement, and simple to operate. Fewer indeterminate results were also seen, as well as superior sensitivity and specificity compared to total serum B12 testing8,9,10.
Another key reason for using Active-B12 as a first-line screen is because this metabolically active portion of vitamin B12 is the earliest laboratory parameter to become decreased if there is depletion due to negative balance of this crucial vitamin. Clinical or haematological symptoms may not yet be present. Other biomarkers can be used to assess Vitamin B12 status - methylmalonic acid (MMA) and homocysteine (tHcy) - which are functional vitamin B12 markers that increase due to metabolic processes as vitamin B12 stores are depleted8,11. However, these are indirect markers of vitamin B12 and will therefore show depletion at a later stage than Active-B12, which is a direct marker and therefore more effective.
Studies have also demonstrated the effectiveness of Active-B12 (HoloTC) when compared to MMA and tHcy8,9,11. For example, in a study of Vitamin B12 status in the elderly it was concluded that HoloTC performed significantly better than other indicators11. Not only is Active-B12 proven to be a sensitive and specific direct marker of Vitamin B12 deficiency, it is easy to use and can be performed on a routine clinical chemistry analyser. Analysis of MMA and tHcy involve more specialised analyses, with MMA requiring mass spectrometry, which is a complex and manual method that often requires samples to be sent to specialized centres for analysis.
Summary
With the worldwide prevalence of anaemia so high, the development and adoption of Active-B12 testing is key. Moving to Active-B12 testing helps to simplify the testing process, aiding in patient diagnosis to initiate treatment faster. In addition, the results from Active-B12 testing present a more accurate representation of vitamin B12 deficiency and anaemia status compared to other tests available, including total serum B12.
Commenting on the new Beckman Coulter Access Active-B12 assay for vitamin deficient anaemia Heather Read-Harper – Senior Marketing Manager, Beckman Coulter observed: “This new addition to our anaemia testing portfolio highlights the Company’s commitment to improving patient care. With the largest measuring range on the market, fastest time to first result and standardisation to WHO International Standard (IS) 03/178, the Access Active-B12 assay provides the final piece in the puzzle for anaemia disease-state management. The comprehensive menu of testing options we provide helps our customers to tackle the complex challenge of anaemia diagnosis. And with proven expertise in analysing laboratory test processes, we work together to understand requirements and create flexible solutions that meet the evolving needs of our customer.”
References
1. Global anaemia prevalence and number of individuals affected. World Health Organization. http://www.who.int/vmnis/anaemia/prevalence/summary/anaemia_data_status_....
2. de Benoist, B et al., eds. Worldwide prevalence of anaemia 1993-2005. WHO Global Database on Anaemia. Geneva, World Health Organization, 2008.
3. Anaemia prevention and control. World Health Organization. https://www.who.int/medical_devices/initiatives/anaemia_control/en/
4. Guralnik, JM et al. Prevalence of anemia in persons 65 years and older in the United States: evidence for a high rate of unexplained anemia. Blood (2004) 104:2263-2268
5. Stoltzfus, RJ. Iron-deficiency anaemia: reexamining the nature and magnitude of the public health problem. Summary: implications for research and programs. Journal of Nutrition (2001), 131(Suppl. 2):697S–701S
6. Surgical care at the district hospital. Geneva, World Health Organization, 2003. https://www.who.int/surgery/publications/en/SCDH.pdf
7. Smith, Jr., R. The Clinical and Economic Burden of Anemia. Am J Manag Care (2010) 16:S59-S66.
8. Herrmann, W and Obeid, R. Holotranscobalamin – An Early Marker for Laboratory Diagnosis of Vitamin B12 Deficiency. European Haematology (2009) 3(1):7-11
9. Valente, E et al. Diagnostic Accuracy of Holotranscobalamin, Methylmalonic Acid, Serum Cobalamin, and Other Indicators of Tissue Vitamin B12 Status in the Elderly. Clinical Chemistry (2011) 57:6 856-863
10. Herrmann, W et al. Vitamin B12—cobalamin, In: Herrman W, Obeid R, eds. Vitamins in the prevention of human diseases. Berlin: De Gruyter (2011)187–99.
11. Nexo, E and Hoffman-Lucke, E. Holotranscobalamin, a marker of vitamin B12 status: analytical aspects and clinical utility. Am J Clin Nutr (2011) 94(1): 359S–365S



