The Serious Hazards of Transfusion (SHOT) scheme collects and analyses anonymised information reported
in the UK about serious adverse reactions and events (SAE) related to blood transfusion, then makes recommendations to improve patient and transfusion safety.

In 2015 SHOT introduced a chapter on donor vigilance provided by the four UK Blood Services, demonstrating the full reach of haemovigilance from donor to recipient. This year SHOT celebrated its 20th anniversary alongside the release of its 2016 Annual Report summarised here.
SHOT recommendations
1. Use a bedside checklist. This will prevent administration errors and is the final opportunity to detect errors made earlier. The checklist must include positive patient identification, and confirm that the component is correct, meets any specific requirements, and that it has been prescribed for the patient at the time. Whatever bedside system is in place (including electronic systems), it should be assessed and include a validation step where someone has to sign to say that all steps have been followed and completed correctly.
2. Use a TACO checklist. Patients should be formally assessed for their risk of transfusion-associated circulatory overload (TACO) whenever possible, since TACO is the most commonly reported cause of death and major morbidity.
Lab recommendations
Laboratories should always have adequate staffing at the appropriate grade to support those that require training.
Appropriate use and management of laboratory information management systems (LIMS) is essential for safety.
Gap analysis should be performed against national transfusion guidelines, and SOPs amended to correct deficiencies.
Deaths and major morbidity
In 2016 there were 26 deaths related to transfusion (possibly, probably or definitely), 16 of which were considered preventable. Of these, 14 were attributed to TACO – double that of 2015. Delays in transfusion contributed to nine deaths
in 2016, compared to six in 2015.
Cumulative data from 2010 to 2016 show that pulmonary complications are overall the leading cause of death, accounting for 61 of 115, and delayed transfusion accounting for 25 of 115.
The SHOT numbers translate into a risk of death of one in 100,000, a risk of death from error of one in 250,000 and a risk of major morbidity of one in 20,400 blood components issued.
Three ABO-incompatible red cell transfusions were reported in 2016, two
of which resulted in major morbidity, but no deaths. Two of these were caused by wrong blood in tube incidents where the two-sample policy was not adhered to. The third was a combination of collection and administration errors which could have been detected had the final bedside administration check been performed. Three ABO-incompatible fresh frozen plasma infusions (now also considered “never events”) were also reported all due to laboratory errors, in testing (1/3) and component selection (2/3).
A patient in sickle cell crisis received serologically crossmatch-incompatible units due to a labelling error, but fortunately experienced no adverse reaction. A further 264 potential ABO-incompatible transfusions were avoided because errors were detected prior to transfusion.
Incidents and reactions
There was one transmission of infection (hepatitis E virus) reported in 2016 (in nearly 2.5 million components issued). There were no cases of transfusion-related lung injury, transfusion-associated graft versus host disease or post-transfusion purpura. Adverse reactions were reported in a total of 385 cases (12.5% of all reports) with allergic, hypotensive and severe febrile reactions continuing to be the most common.
There were 35 cases of acute haemolytic transfusion reactions (AHTR), and five delayed haemolytic transfusion reactions were reported this year. One patient with sickle cell disease (SCD) died related to hyperhaemolysis. There were seven cases of major morbidity, five with hyperhaemolysis in patients with SCD. Four in 17 cases of AHTR involved the presence of antibodies to low-frequency antigens on red cells that were electronically issued. One was attributable to anti-Wra.
Key findings
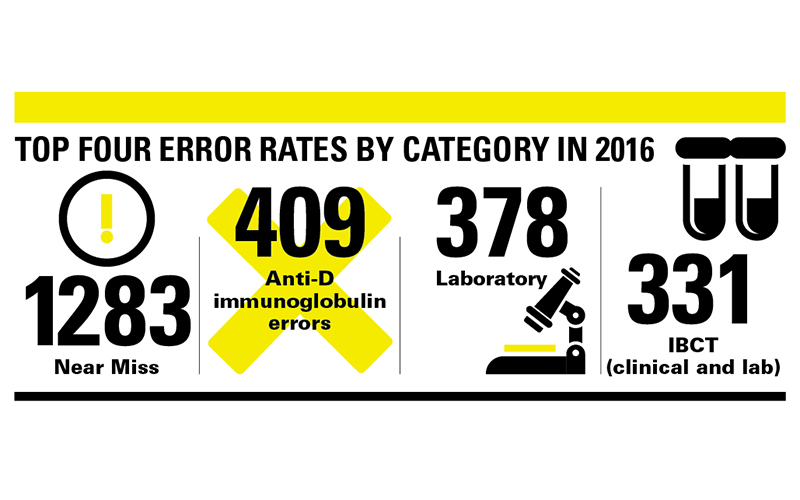
Reports related to human error have increased to 2688/3091, 87% (2015: 2555/3288, 78%). There were 1,510 errors that resulted in either a near miss or right blood to right patient (RBRP) that caused no harm. 1,178 reported errors led to actual or potential harm comprising handling and storage errors (HSE), avoidable and delayed transfusions, anti-D immunoglobulin errors and incorrect blood components transfused (IBCT).
There have been increases in testing and component selection errors in the laboratory reported since 2015. Understaffing, poor knowledge and skills and high workloads feature in many of the reports, consistent with findings from the 2015 UK Transfusion Laboratory Collaborative (UKTLC) survey.
IT-related errors contributed to one in five of the SAE reported jointly to SHOT and the MHRA. These include transcription errors resulting in incorrect patient demographic details and incorrect results entered onto the LIMS, failure to heed warning flags, and poor LIMS control of component selection and electronic issue suitability. A total of 20 cases were reported this year where blood was issued electronically when the patient was not eligible.
Most near-miss errors result from inadequate patient identification at sample-taking and blood component administration. Increasingly errors are occurring with transplants, with 93 reports in 2016 compared with 70 in 2015. Nineteen of 58 haemopoietic stem cell transplant errors and four of 35 solid organ transplant errors were ABO- and/or D-related. These could have been prevented by effective communication from clinicians to the laboratory or by the laboratory heeding the historical LIMS record.
Human error
A human factors investigation tool was added to the SHOT (Dendrite) database in January 2016, asking the reporter to examine the extent to which four human factors were implicated in each incident:
- Unsafe practice by individuals
- Unsafe conditions associated with the local environment or workspace
- Unsafe conditions associated with organisation or management
- Conditions associated with the government, Department of Health or high-level regulatory issues.
The 2015 UKTLC survey reported that 90/204 (44.1%) of transfusion laboratories had vacant posts, 43 of these employed agency staff and 100/178 (56.2%) laboratories were involved in reorganisation. It is often easier to blame the individual than to look at the organisational circumstances that contributed to the error. A self-learning package is available on the SHOT website. Blood components are very safe but we must continue to learn from errors and improve our practice.
Jenny Berryman is a Specialist Advisory Panel Representative (Transfusion),
Hema Mistry is a Laboratory Incidents Specialist and Paula HB Bolton-Maggs is Medical Director, all at SHOT.



